Massachusetts Patient Sentiment toward Non-Medical Drug Switching
Background
Although formularies and other utilization management techniques may help contain costs for third-party payers, potential savings often come at the expense of patients’ health. One major example is non-medical switching, which occurs when a health plan’s formulary changes in a way that monetarily pressures patients to cease filling their prescribed medication in lieu of a “preferred” or cheaper drug. Non-medical switching can occur during the health plan year.
Formulary changes may include:
- Completely removing a patient’s medication from the formulary;
- Increasing the patient’s out-of-pocket costs;
- Changing the tier of the patient’s drug or adding new restrictions on the medication.
Formulary changes can happen at any time. Insurers are free to change formulary coverage however they wish, whenever they wish. Changes often occur mid-year and it is important to understand that patients cannot renegotiate their contracts mid-plan and therefore have no choice but to stay with the plan. Essentially, patients are not being provided with the benefits that were marketed to them during the open enrollment period. Whatever form it takes and whenever it occurs, non-medical switching can be very harmful to patients. As a result of being switched from their original, clinician-prescribed medication, patients may experience additional side effects, symptoms, disease progression, and potentially relapse. Beyond the immeasurable impact of this unnecessary suffering, the negative effects of non-medical switching can result in additional medical appointments, emergency room visits and even hospitalization, thereby actually increasing overall healthcare utilization costs. Despite this, the impact of non-medical switching on patients has been remarkably unmeasured and ignored by health insurance and pharmacy benefit management companies. In order to better understand how Massachusetts patients are affected by this harmful utilization management technique, Global Healthy Living Foundation (www.ghlf.org) conducted a survey of Massachusetts residents living with chronic diseases.
The survey’s aim was two-fold in measuring:
- The prevalence of Massachusetts residents who are living with chronic diseases being pressured to switch from their clinician-prescribed medicine for non-medical reasons; and
- The adverse physical, mental, emotional, and productivity impact of non-medical switching.
Methodolgy
From August through October 2017, GHLF partnered with the Massachusetts Patient Access and Safety Coalition, which consists of 19 diverse patient and clinician advocacy organizations representing hundreds of thousands of residents in Massachusetts living with chronic illness and their care providers. GHLF and the Massachusetts Patient Access and Safety Coalition invited Massachusetts residents living with a chronic or rare illness to complete an online, 31-item survey that investigated patient experiences with the manipulation of their respective health plans’ formularies.
In order to complete the survey, eligible respondents had to be:
- Diagnosed by a physician with a chronic or rare disease; and
- Currently living in Massachusetts
Prospective respondents who did not meet these two eligibility criteria were disqualified and prevented
from completing the survey.
Executive Summary
A total of 260 Massachusetts residents started the online survey. Forty of the 260 participants did not complete the survey and 77 were disqualified for either not having a chronic or rare disease or for not experiencing a non-medical switch. The total number of participants who completed the survey is 143; only completed responses were analyzed. Although respondents’ individual diseases varied widely, five separate major classes were represented: mental health (35%), autoimmune (34%), neurological (29%), oncological (6%) and infectious (1%). A majority were female (73%), white (82%) and college educated (75%). There was an equal percentage (46%) of participants who were employed, either full-time, part-time, or self-employed, as there were participants who were unemployed. The majority of participants (64%) reported having a household income of $50,000 or less per year. All types of insurance coverage were represented in our surveyed population. Private was held by the most number of respondents (43%), followed by public (36%), followed by a combination of private and public insurance (16%).
How many patients does non-medical switching negatively impact?
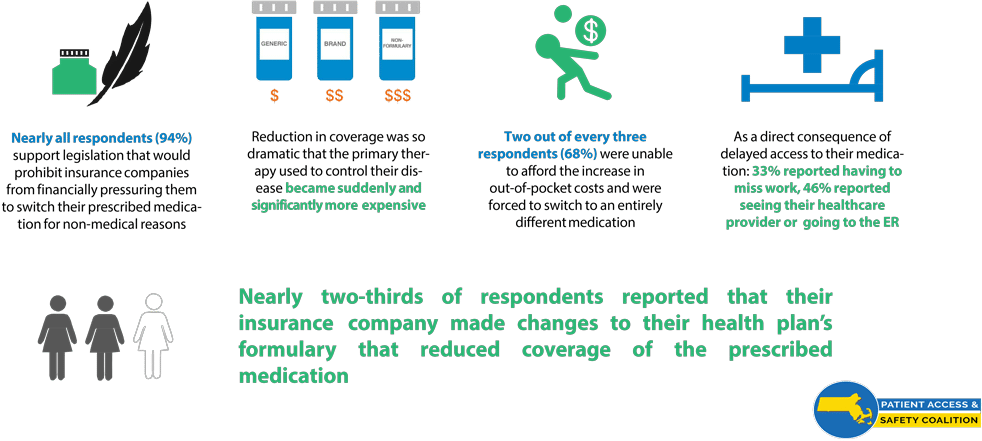
Results of this survey show that it is commonplace for chronic and rare disease patients in Massachusetts to experience sudden decreases in prescription-medication coverage. Almost two-thirds (64%) reported that their insurance company switched their medication to a drug that was different from the one their physician prescribed as the result of a formulary change. As much as 65% of those patients did not have the opportunity to reject and/or decline the medication switch. In addition to forced switches, mid-year changes in insurance coverage have been found to be so dramatic that nearly three-quarters (73%) reported that the primary therapy prescribed to them became suddenly and significantly more expensive to obtain. The majority of respondents (66%) reported now paying more out-of-pocket for their prescribed medication, with 53% reporting to pay a lot more. Overall, effectively, two out of every three (68%) of our survey respondents reported being financially coerced by their insurance companies to change their clinician-prescribed medication for non-medical reasons.
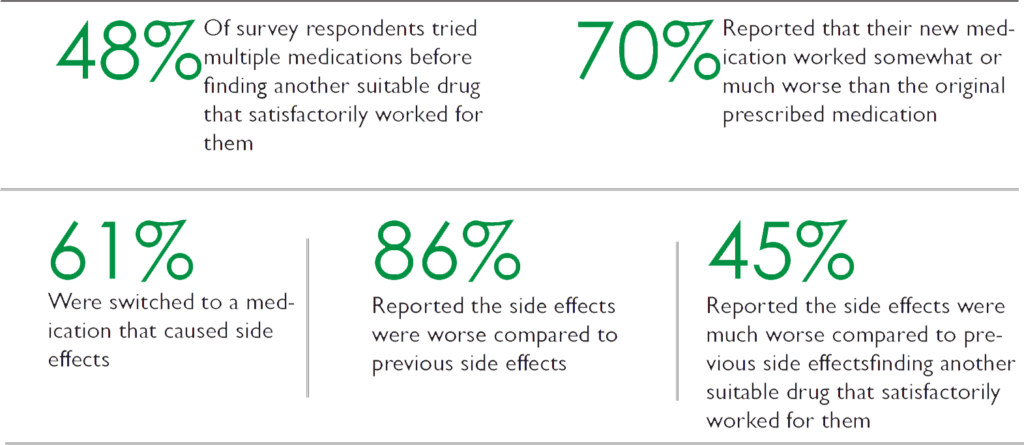
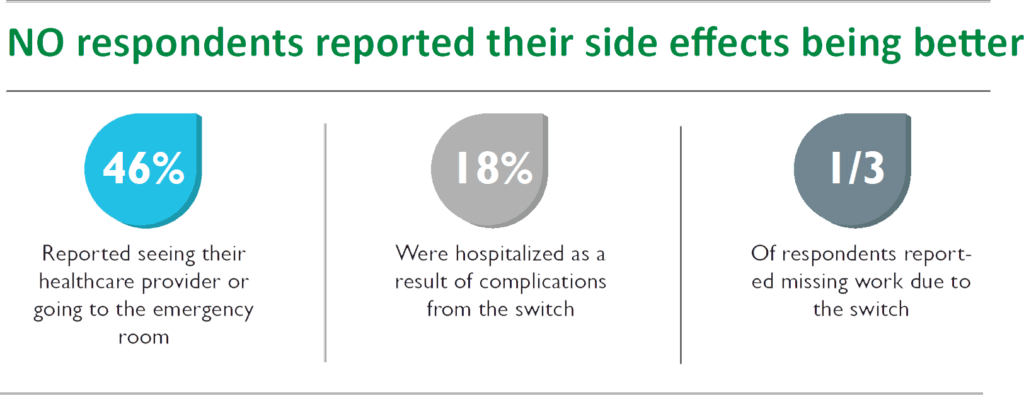
How does non-medical switching impact patient’s treatment and health?
Do insurers properly communicate formulary changes to patients?
When investigating communications by third-party payers to inform patients about formulary changes, our survey found close to half (42%) of all respondents reported never receiving any notifications, such as letters, emails, or phone calls, communicating details of their plan’s formulary or changes being made to it. When respondents experienced alterations to their plan’s formulary, only a quarter (24%) reported their insurance company informed them of the altered coverage to their prescribed medication. A majority of respondents (68%) was informed by their pharmacist, and a small percentage (5%) was informed by their physician.
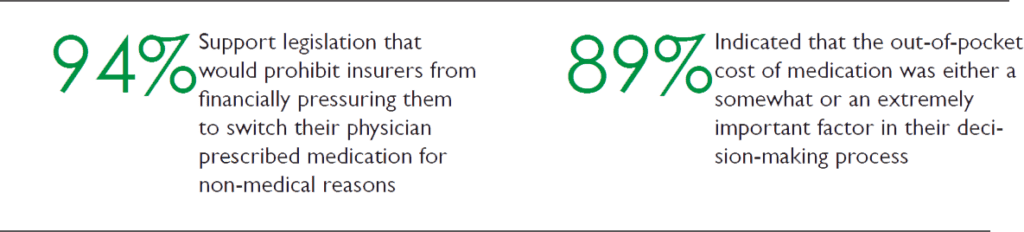
How do patients feel about non-medical switching?
Conclusions and Recommended Policy Action
Our survey has shown that non-medical switching is a prevalent and growing practice in Massachusetts. It can put patients who have complex, chronic, or rare diseases at severe risk. Multiple switches can either force patients onto less effective and more dangerous medications or eliminate treatment options for patients in a disease state that has a limited bank of therapies. Health insurance companies’ utilization management techniques, such as reductions in drug coverage, result in treatment gaps and cessation of effective therapy, which often takes years to find. As a result of associated increases in side effects and adverse reactions that can lead to hospitalization, more doctors’ appointments, emergency room visits, and so on, non-medical switching can actually increase overall utilization costs. Do insurers properly communicate formulary changes to patients? Currently, there are no state protections for patients in Massachusetts from formulary coverage changes that can disrupt effective treatment. Massachusetts needs public policy that protects patients with chronic diseases that are stabilized on therapy from disruptions due to non-medical reasons.